athlete's heart can look like HCM
- related: heart failure
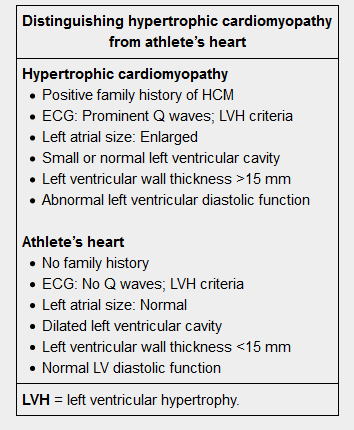
This patient's ECG findings – high-voltage QRS complexes and lateral repolarization abnormalities (inverted T waves) – are consistent with left ventricular hypertrophy (LVH). Young (age <35) athletes can develop a physiologic increase in left ventricular wall thickness, cavity size, and myocardial mass in response to intense cardiovascular training. This physiologic condition, termed athlete's heart, can lead to findings of LVH on ECG in the absence of any cardiovascular pathology. However, hypertrophic cardiomyopathy (HCM), the most common cause of sudden cardiac death (SCD) in young athletes in the United States, usually causes similar findings on ECG. In addition, approximately 20% of patients with HCM present with episodes of presyncope.
Because absence of a systolic ejection murmur on physical examination does not rule out HCM, a young athlete such as this patient with ECG findings of LVH and unexplained symptoms (eg, chest pain, palpitations, presyncope, syncope) should be evaluated for HCM or other structural heart disease (eg, aortic stenosis) with transthoracic echocardiography. Left ventricular wall thickness <15 mm, among other clinical characteristics, can help distinguish athlete's heart from HCM.